1. Background
1.1. 3D-images
In radiation therapy, medical body scans are an important tool which doctors can use for planning dosage delivery. Several different modalities of scans are used, including:
Computed Tomography (CT) scans. These essentially take cross-sectional slices (tomograms) and that can be used in computing a reconstruction of the full 3D-image. CT-scans typically indicate air with a value of -1000, water with 0, and bone with 400 or greater (measured in Hounsfield units).
Positron emission tomography (PET/PT) scans. These utilise gamma rays to visualise injected radiotracers, which are essentially compounds that are radioactively decaying in such a way that the PT-scan can show the spatial journey of the compounds during a scan. Many different radiotracers exist, e.g. for metabolism and blood flow tracing, and the way in which a PT-scan visualises compounds depends on the choice of radiotracer and the chosen task.
Magnetic Resonance (MR) scans. These use magnetic resonance to visualise body tissue and other substances and come in two types: T1-MR and T2-MR, which measure different kinds of magnetic resonance. They typically indicate bone and air with values close to 0 and fat with higher values, while the visualisation values of water, protein-rich fluids etc. depend on the type used.
In general, medical scans consist of 3D-images, which differentiates them from regular 2D-images. 2D-images have grids that consist of pixels. A pixel is defined by the (x,y) coordinates of its centre along with a colour value. The size of a pixel is defined by the length of the pixel multiplied by the height of the pixel. In the case of 3D-images, a voxel is defined by the (x,y,z) coordinates of its centre along with a colour value. Likewise, the size of a voxel is defined by the voxel’s length, height and depth multiplied together. The colour values of medical scans typically lie on a greyscale range based on the modality of scan, i.e. voxels that show air will have a value of -1000 in CT-scans and a value of around 0 in MR-scans, as described above.
All three modalities of medical scans along with medical information are stored in the so-called DICOM-format from the beginning. DICOM is an acronym for Digital Imaging and Communications in Medicine. It is a file format that stores digital 2D-images. Since medical scans are 3D-images, you often need hundreds of DICOM files to represent a single scan. Additionally, DICOM-files can also store medical information, e.g. descriptions of the scans. Finally, DICOM-files are even able to store delineations, which are essentially medical hand-drawn outlines of where organs and tumours are located. These delineations are crucial to the planning of the medical treatment, and it is thus the main goal of an ultimate deep learning model to learn to construct these delineations.
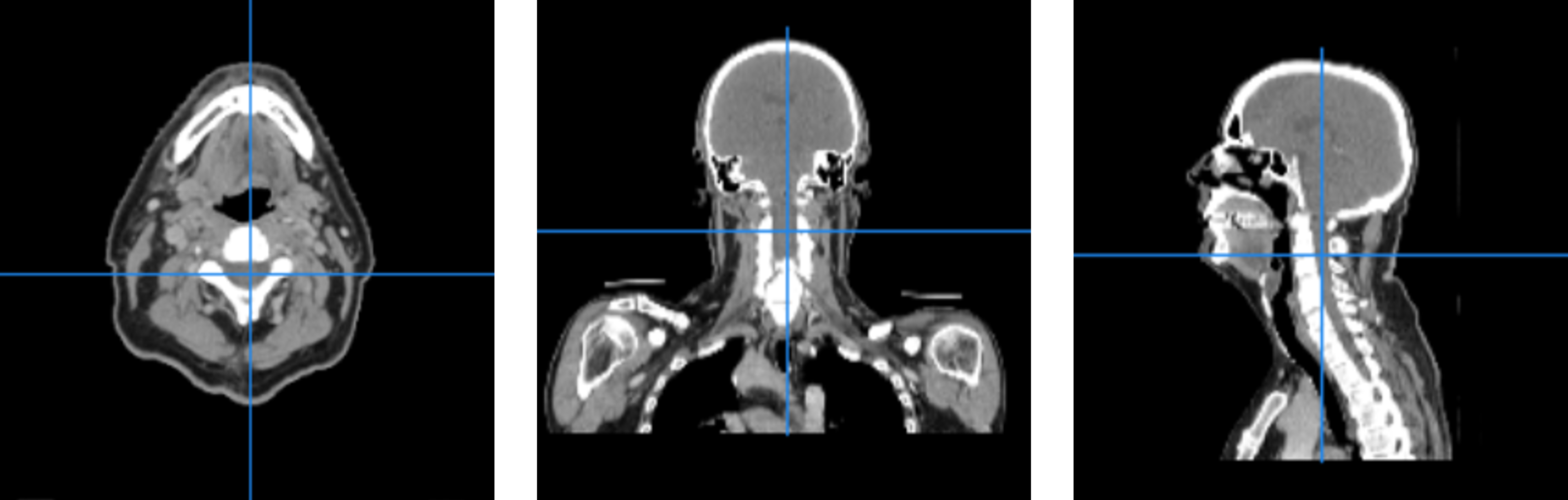
Example of three CT-scan slices in the axial (left), coronal (middle) and sagittal (right) plane. The slices have been zoomed independently for ease of viewing.
Thus, DICOM-files ensure that all the data for each patient stays with the respective patient. However, in order to make them easier to handle for both doctors and an eventual deep learning model, they need to be converted into a niftier format.
Instead of having a lot of 2D-slices to represent a body part, we want to represent it as a 3D-volume. This is exactly what the Neuroimaging Informatics Technology Initiative (NIfTI) file format accomplishes. This makes it easier to keep all the data together, since there are no longer hundreds of files to manage. In addition to that the NIfTI-file also contains all of the medical information. These NIfTI-files can also be used as input for a deep learning model. In fact, the deep learning framework known as nnU-Net, which is commonly used to automatically tune hyperparameters and train the network in medical image tasks, only accepts NIfTI-formatted 3D-scans, making the format significantly more advantageous than the DICOM-format.
1.2. Registration
When only one modality of scan is used for a deep learning model, simply converting e.g. the CT-scan to NIfTI is sufficient preprocessing. However, when introducing several modalities of scans simultaneously, one must ensure the scans all contain the exact same organs in the exact same areas. E.g. when using both CT-scans and MR-scans as input to the neural network, the MR-scan must be manipulated so that e.g. the mandible is located across the exact same voxels as in the CT-scan. It is typically easier to manipulate the MR-scan, since any delineations are typically created based on the CT-scan and would thus also need to be manipulated.
To ensure the above equivalence, a procedure known as registration must be performed, along with cropping the images in case one scan covers more of the body than the other. Registration is done in two types, whereof the first is called rigid registration. This essentially amounts to rotating and translating the entire MR-scan to fit the CT-scan as well as possible. It can occasionally be difficult to perform sufficient registration using only the rigid method, e.g. if the patient’s jaw was opened a bit more during the MR-scan than in the CT-scan.
The other type of registration, deformable registration, solves exactly this problem. In deformable registration, individual voxel values may be displaced within constraints with respect to the rest of the image, i.e. in the previous example, the lower jaw may be “moved up” to better fit the closed jaw of the CT-scan. This procedure requires a certain level of constraint, since otherwise voxels would be moved erratically. In turn, this means deformable registration should be preceded by rigid registration, so that only small voxel adjustments are necessary.
1.3. Evaluation
After having performed registration, it remains to check that the registrations were performed well. One possible way is to manually check all of the data that has been processed, i.e. visualise the images and look for poor registrations. Often this is time consuming, and sometimes the human eye is not as good at spotting irregularities as computers might be. Therefore, a metric is often used. Metrics measure how well a process was performed, i.e. they often give one or two values that describe how accurately the data was preprocessed. In the case of registration, the “accuracy” is how similar the CT- and MR-images are. Several metrics that measure this kind of 3D-image similarity exist, including:
Correlation coefficient, measuring the correlation between voxel values at identical positions of the two images. Only works within the same modality, since the correlation requires e.g. bone to always be brighter than fat tissue to be appropriate.
Dice coefficient (also known as the Sørensen-Dice coefficient), measuring the quotient between overlapping volume and total volume. The volumes are based on segmentation and/or selected to include only voxels with values above a certain threshold.
Mutual Information, measuring how well a voxel value from one image can be predicted from the same voxel’s value in another image. Is not dependent on direct correlation between voxel values, and is thus useful for comparing scans with different modalities.
Many 3D-image similarity metrics, including the above, suffer from an issue wherein “background” (in this case, air) voxels contribute to false accuracy. This issue can be partially remedied by cropping the image to include as little air as possible. In addition to that, they also require the images to have the same size, since “something” cannot be compared with “nothing”.